DEA Requirements for Nurse Practitioners: What You Need to Know in 2026
Controlled-substance prescribing is part of everyday care for many nurse practitioners, but the rules are easy to get wrong. Whether you’re managing chronic pain, treating ADHD, or addressing anxiety disorders, your ability to prescribe Schedule II–V medications depends on getting and maintaining the right DEA registration.
The process is not just a federal form. NPs also have to account for the 8-hour training rule, state controlled-substance credentials, and, in many states, a collaborative agreement with a physician who has DEA authority.
This guide walks through the main DEA issues NPs need to understand in 2026:
- The 8-hour federal training mandate that took effect in 2023
- Step-by-step instructions for obtaining your DEA registration
- How state laws intersect with federal DEA requirements
- The critical connection between DEA compliance and collaborative agreements
- Current rules on multi-state DEA registration for telemedicine and collaborating physicians
Whether you’re starting an independent practice, expanding into new states, launching a telehealth service, or simply renewing your DEA registration, this article will help you stay compliant and avoid costly delays.
DEA Requirements for NPs at a Glance
What Is DEA Registration and Why Do NPs Need It?
DEA registration is a federal authorization to prescribe, administer, or dispense controlled substances under the Controlled Substances Act (CSA). Administered by the Drug Enforcement Administration (DEA), this registration provides you with a unique DEA number that pharmacies require before filling prescriptions for controlled medications.
When You Need a DEA Number
You need a DEA registration if you prescribe:
- Schedule II medications: Opioids (oxycodone, hydrocodone, fentanyl), stimulants (Adderall, Ritalin), short-acting barbiturates
- Schedule III medications: Codeine combinations, ketamine, anabolic steroids, buprenorphine
- Schedule IV medications: Benzodiazepines (Xanax, Ativan, Valium), Ambien, tramadol
- Schedule V medications: Low-dose codeine preparations, pregabalin
You do not need a DEA number for non-controlled medications like antibiotics, blood pressure medications, antidepressants, or diabetes medications.
The Three Layers of DEA Compliance
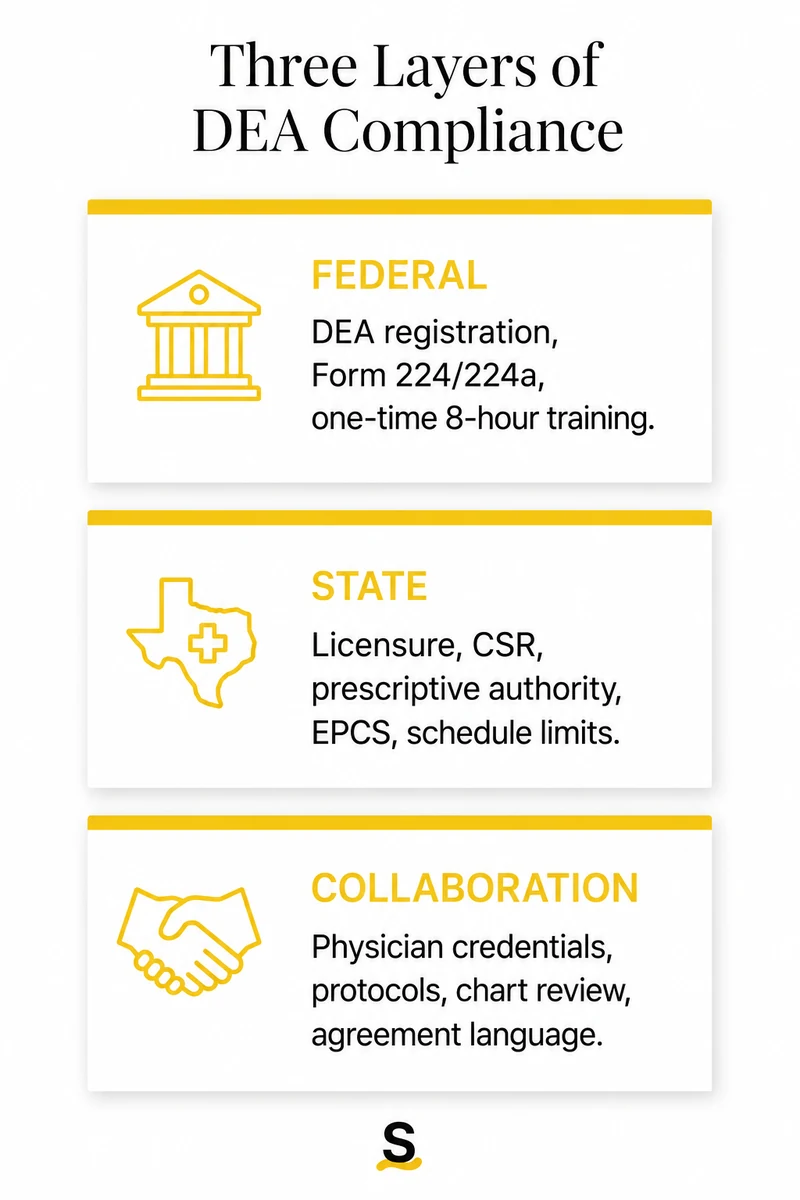
It helps to separate DEA compliance for NPs into three layers. Confusion usually starts when these get treated as one system.
The federal layer is your DEA registration itself, plus the one-time 8-hour training requirement under the Consolidated Appropriations Act. This is the one layer that is mostly uniform nationwide.
The state layer is where most variation lives: state controlled substance registrations (CSRs), state prescriptive authority rules, electronic prescribing mandates, and state-specific limits on which schedules you can prescribe. A federal DEA number doesn’t override state requirements, you have to satisfy both.
The collaboration layer applies in states that require physician collaboration or supervision for NP prescriptive authority. In those states, your ability to prescribe controlled substances depends not just on your own credentials but on your collaborating physician’s credentials and the language in your collaborative practice agreement.
The rest of the article moves through those layers, then turns to telemedicine and cross-state collaboration.
The 8-Hour DEA Training Requirement
As of June 27, 2023, DEA-registered practitioners, including nurse practitioners and other non-veterinarian practitioners who are legally authorized by state law to dispense Schedule II–V controlled substances, must satisfy a one-time 8-hour training requirement1 on treating and managing patients with opioid or other substance use disorders.
What You Need to Know
Training generally needs to cover:
- Treatment and management of opioid and substance use disorders
- Pain management and responsible opioid prescribing
- Screening, brief intervention, and referral for treatment
- Overdose prevention and naloxone distribution
When it’s required: You must affirm completion on your next DEA registration submission after June 27, 2023, whether that’s an initial application or a renewal.
One-time only: Once you’ve affirmed the training requirement, you don’t need to repeat it for subsequent renewals.
No specific course required: The DEA does not mandate one particular 8-hour course. You can use qualifying past training or combine eligible continuing education activities, online modules, webinars, and conference sessions from organizations recognized in the statute or DEA guidance. NPs often satisfy the requirement through:
- DATA 2000 Waiver training (if completed and relevant)
- AANP-approved CE courses on addiction and pain management
- SAMHSA-approved training programs
- Accredited medical education on opioid use disorder
Exemptions
You’re exempt from the 8-hour training if:
- You’re board-certified in addiction medicine or addiction psychiatry
- You graduated from an accredited NP program within the past 5 years that included substance use disorder training in its curriculum
Documentation
Keep records of your training. While the DEA doesn’t require you to submit certificates with your application, you must be able to provide documentation if audited. Save:
- Course completion certificates
- CE credit records
- Program descriptions showing opioid/SUD content
State Requirements That Affect DEA Compliance
Federal DEA registration is only the starting point. The harder operational questions usually come from state law.
State Prescriptive Authority Varies Widely
Having a DEA number does not automatically grant prescriptive authority in every state or setting. DEA registration depends on state authority, and state boards of nursing, pharmacy boards, and medical boards may require:
- A separate state-level controlled substance license
- Collaborative practice agreements with physicians
- Additional training or certification
- Protocol agreements for specific medication classes
A few examples of how state requirements differ:
- Texas NPs need a Prescriptive Authority Agreement with a physician
- California NPs typically need a furnishing number and standardized procedures to prescribe controlled substances, unless practicing under the state’s independent practice authority (AB 890)
- Georgia NPs require a collaborative agreement that specifically addresses controlled substance protocols
- Florida APRNs generally practice under an established protocol unless autonomous-practice registration applies; controlled-substance prescribing also depends on graduate preparation and specialty/scope limits
State Controlled Substance Permits (CSRs)
Beyond your NP license, some states require a separate state-level controlled substance license or permit. This is typically obtained from your state’s Board of Pharmacy or a dedicated controlled substance authority.
You must have this state permit before applying for federal DEA registration. Without it, your federal application will be denied or delayed.
Currently 25 jurisdictions require this second license, including states like Illinois, Michigan, and New Jersey. The DEA maintains the current list on its Practitioner’s State License Requirements page3.
Check requirements with your state’s Board of Nursing, Board of Pharmacy, or controlled-substance authority.
Collaborative Agreement Requirements
If you practice in a state requiring physician collaboration, your collaborative practice agreement is the legal foundation for controlled substance prescribing. DEA compliance and collaborative agreements must be reviewed together.
What Your Collaborating Physician Must Have
In many states, your ability to prescribe controlled substances depends on having a collaborative practice agreement with a physician who:
- Has active DEA registration with authority to prescribe controlled substances
- Is licensed in your practice state
- Has explicitly authorized controlled substance prescribing in your collaborative agreement
The collaborating physician must be legally authorized to prescribe controlled substances themselves before they can authorize that prescribing under your collaborative agreement. This means verifying:
- Their DEA registration is current (not expired or suspended)
- Their state medical license permits controlled substance prescribing
- They have any required state-specific controlled substance licenses
- Your collaborative agreement explicitly addresses protocols for controlled substance prescribing, including chart review requirements and prescribing limitations
What Your Collaborative Agreement Must Address
Your agreement should specify:
- Which drug schedules you’re authorized to prescribe
- Protocols for pain management and opioid prescribing
- Chart review requirements for controlled substances
- Prescribing limitations (quantity limits, refill policies)
- Emergency prescribing procedures
Example: In Texas, the Prescriptive Authority Agreement must specify protocols for prescribing controlled substances, including limitations on drug schedules, quantities, and refill policies.
Why This Matters: A Common Pitfall
NPs sometimes obtain DEA registration but discover their collaborative agreement doesn’t authorize controlled substance prescribing, or their collaborating physician lacks DEA authority in the required state.
The result is frustrating: you may have a DEA number that does not work for the practice you are trying to operate. That creates compliance risk, business delay, and patient-care friction.
Before applying for DEA, confirm that the collaborative agreement, the physician’s credentials, and the state’s controlled-substance rules line up.
Need help finding a collaborating physician with appropriate state licensure, DEA registration, and controlled-substance experience? Single Aim connects NPs directly with physicians who can support state-specific collaboration and prescriptive-authority requirements.
Multi-State Considerations
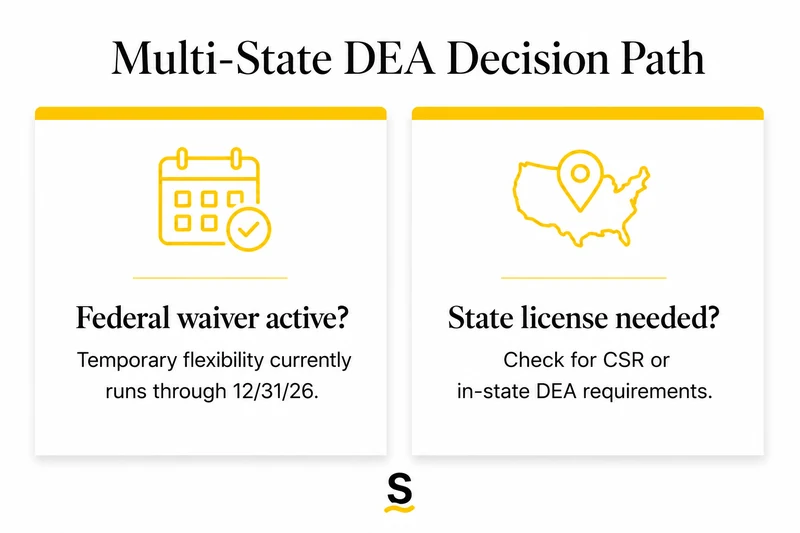
Cross-state practice creates two separate questions: whether the temporary federal flexibility applies, and whether the state has its own in-state DEA or controlled-substance requirement.
The Multi-State DEA Waiver
In March 2020, in response to the COVID-19 public health emergency, the DEA issued a temporary exception waiving the requirement to obtain a separate DEA registration4 in each state where prescribing occurs, as long as the practitioner is authorized to prescribe controlled substances in both states.
Current status: The waiver is set to expire December 31, 20265, but it has been extended four times already.
What this means: As long as the federal waiver remains in effect, a collaborating physician with a DEA registration in one state can support controlled-substance prescribing for NPs in other states without obtaining a separate DEA registration in each state. This applies only if the physician is authorized to prescribe controlled substances in both states, and the practice state doesn’t require an in-state DEA registration.
Proposed telemedicine DEA registration: The DEA has proposed a formal "telemedicine DEA registration" process that would provide a permanent framework for multi-state prescribing, but as of this review it has not yet been enacted.
In-State DEA Registration Requirements
Here is the practical distinction: although the current federal exception allows a practitioner with a DEA registration in one state to prescribe in others without obtaining additional DEA registrations, some states explicitly require an in-state DEA registration to prescribe controlled substances within their borders, overriding that flexibility.
States that currently require in-state DEA registration include:
- Delaware: "You must have both a Delaware CSR and DEA registration for Delaware6 before you prescribe controlled substances in Delaware. A DEA registration in another jurisdiction is not sufficient."
- Idaho
- Nevada
- South Dakota
- Alabama
If you’re practicing in one of these states, or if your collaborating physician is based in one of these states, verify the in-state DEA requirement.
Heuristic for Multi-State Collaborating Physicians
When working with a collaborating physician who supports your controlled substance prescribing across multiple states, use this framework:
The collaborating physician must:
- Be authorized to prescribe controlled substances in your practice state under that state’s law (typically requiring an active medical license and any state controlled substance registration that state requires)
- Be permitted under your practice state’s collaboration or supervision rules to serve as your collaborating physician for controlled substance prescribing
DEA registration considerations:
- As long as the federal waiver remains in effect, the collaborating physician does not need to obtain a separate DEA registration in each state where you prescribe, provided they are authorized to prescribe controlled substances in both their home state and your practice state
- Exception: If your practice state explicitly requires an in-state DEA registration (DE, ID, NV, SD, AL), the collaborating physician must have a DEA registration tied to that state regardless of the federal waiver
Watch this closely: The December 31, 2026 expiration date could significantly impact telemedicine and multi-state collaboration arrangements. If the waiver expires without replacement, collaborating physicians may need separate DEA registrations in each state where they serve as a collaborating physician for controlled substance prescribing.
How to Get a DEA Number as a Nurse Practitioner
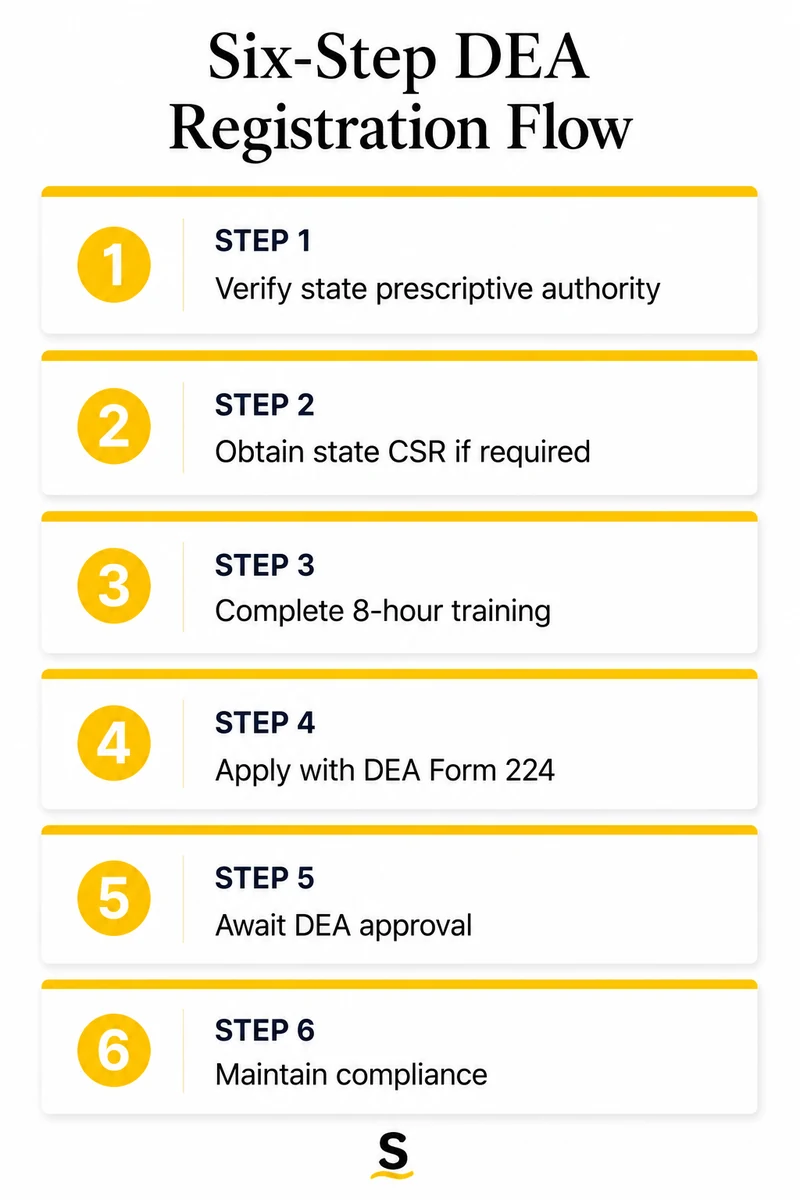
Step 1: Verify State Prescriptive Authority
Before applying for federal DEA registration, confirm:
- An active, unrestricted NP license
- Prescriptive authority in the state
- Any required state controlled-substance registration
- Any required agreement, protocol, or delegation language for controlled substances
In restricted-practice states, you’ll need a collaborative practice agreement in place before you can legally use your DEA registration. Your collaborating physician must have DEA authority in the state where you’re prescribing.
Step 2: Obtain State Controlled Substance License (If Required)
Many states require a separate state-level controlled substance registration before you can apply for federal DEA registration. This is distinct from your NP license. See the State Requirements section above for examples of states that require this step.
In many states, the federal application cannot move forward until the state registration is active.
Step 3: Complete the 8-Hour Training Requirement
Complete qualifying continuing education activities on opioid and substance use disorder treatment. Retain documentation, course certificates, CE credits, and program descriptions for your records.
You’ll affirm completion during the DEA application process, but you won’t submit certificates unless audited.
Step 4: Apply for DEA Registration
Complete DEA Form 224 online through the DEA Diversion Control Division website.
You’ll need to provide:
- Personal and professional information (name, license number, NPI)
- State NP license details
- State controlled substance registration number (if applicable)
- Business address where you’ll be prescribing
- Drug schedules you intend to prescribe (typically Schedule II–V)
- Affirmation of 8-hour training completion
- Application fee: $888 (as of 2026)2
- Payment: Credit card, electronic check, or money order
Step 5: Await DEA Approval
The DEA reviews your application and verifies:
- State license validity
- State controlled substance registration (if required)
- Training affirmation
- Background information
- Typical processing time: 4–6 weeks
- Expedited processing: Not available for new applications. Plan ahead. Do not wait until you need to prescribe to start the process.
Step 6: Maintain Compliance
Once you receive your DEA certificate:
Keep it secure: Store your DEA certificate in a safe location; never share your DEA number publicly
Update address changes: If you change practice locations, update your registration within 30 days
Renew on time: DEA registration expires every 3 years; renewal requires DEA Form 224a
Monitor state requirements: State rules can change; stay current with your Board of Nursing updates
Record-Keeping and Security Requirements
A DEA number also creates ongoing compliance work.
Record-Keeping Requirements
The DEA requires you to maintain accurate records of all controlled substance prescriptions, including:
- Patient name, address, and date of birth
- Medication name, strength, and dosage form
- Quantity prescribed
- Number of refills authorized
- Date of prescription
- Prescriber signature (or electronic equivalent)
Records must be readily available for DEA inspection for at least 2 years (some states require longer retention).
Security Protocols
Protect your DEA registration and prescribing systems:
- Secure prescription pads: If you use paper prescriptions, store them in a locked area; never leave them accessible
- Electronic prescribing security: Use strong passwords, enable two-factor authentication, and limit access to authorized users only
- Monitor for theft or loss: If your DEA number is compromised, report it to the DEA immediately
Electronic Prescribing for Controlled Substances (EPCS)
Many states now require electronic prescribing for controlled substances. EPCS systems must meet strict DEA security requirements, including:
- Two-factor authentication for prescribers
- Audit trails for all prescriptions
- Secure prescription transmission to pharmacies
Check your state’s EPCS requirements. Even when it is not required, EPCS can reduce prescription fraud and make prescribing easier to audit.
Frequently Asked Questions
Can a nurse practitioner prescribe controlled substances without a DEA number?
No. Federal law requires all practitioners, including NPs, to have a DEA registration to prescribe any medication classified as a controlled substance (Schedule II–V). Non-controlled medications do not require DEA registration.
How long does it take to get a DEA number?
Typically 4–6 weeks after submitting DEA Form 224, assuming all documentation is complete and accurate. Delays occur if:
- Your state controlled substance license isn’t active
- You haven’t affirmed the 8-hour training requirement
- There are discrepancies in your application information
Plan ahead: don’t wait until you need to prescribe to start the process.
Do I need a separate DEA number for each state I practice in?
Generally, not while the current federal flexibility is in effect through December 31, 2026, as long as you are authorized to prescribe controlled substances in both the DEA-registration state and the state where prescribing occurs. See the Multi-State Considerations section above for the full picture, including the in-state DEA exception states (DE, ID, NV, SD, AL).
What happens if I don’t complete the 8-hour training?
You cannot affirm compliance on your DEA registration application or renewal. Without affirmation, the DEA will not process your registration. Your application will be returned or denied.
Complete the training before submitting your DEA application or renewal.
Does my collaborating physician need a DEA number for me to prescribe controlled substances?
In states requiring collaboration for controlled substances, yes. See the Collaborative Agreement Requirements section above for the full list of what your collaborating physician must have, including active DEA registration, a state medical license in your practice state, and authority under state law to authorize controlled substance prescribing through a collaborative agreement.
Can I use my DEA number immediately after approval?
Yes, once your DEA registration is approved, you can begin prescribing controlled substances immediately, provided:
- Your state controlled substance license is active
- Your collaborative agreement authorizes controlled substance prescribing (if required in your state)
- Your collaborating physician has appropriate DEA authority (if required in your state)
Finding a Collaborating Physician for Controlled Substance Compliance
In restricted-practice states, DEA registration is only half the problem. You need a collaborating physician with DEA authority before you can prescribe controlled substances to patients.
Finding the right match quickly is important, especially if you’re:
- Starting a new independent practice
- Expanding into a new state
- Launching a telemedicine service
- Replacing an unresponsive or expensive collaborating physician
How Single Aim Helps
Single Aim connects nurse practitioners directly with collaborating physicians. Here’s what makes us different:
Direct connections: Physicians set their own terms, transparent pricing, you control the relationship
State-specific compliance resources: Access CPA templates, state requirement guides, and FAQ hubs for all states
Network coverage: Find a collaborating physician licensed in your state with appropriate DEA authority for controlled substance prescribing
Fast matching: Often connected within 24 hours
Cost transparency: No hidden fees or monthly retainers, just fair, direct pricing
Whether you’re applying for your first DEA registration or expanding into a new state, having the right collaborating physician in place is important. Single Aim connects you directly with qualified physicians who can support your controlled substance prescribing needs, with clear protocols, responsive oversight, and full compliance.
Compliance Disclaimer
Note: The information in this article is for informational purposes only and is not intended as legal or regulatory advice. DEA regulations are federal, but state requirements vary significantly and are subject to change. The multi-state DEA waiver discussed in this article is temporary and set to expire December 31, 20265, though it has been extended multiple times. Please consult your state’s Board of Nursing, Board of Pharmacy, and other relevant regulatory authorities to ensure compliance with all applicable requirements. For legal questions specific to your practice, consult with a healthcare attorney licensed in your state.
Citations
- DEA MATE Act training requirement Q&A.
- 21 CFR 1301.13, DEA registration fees and registration periods.
- DEA Practitioner’s State License Requirements.
- DEA March 25, 2020 state reciprocity exception letter.
- DEA/HHS fourth temporary extension of COVID-19 telemedicine flexibilities.
- Delaware APRN controlled-substance registration guidance.
Find Collaboration Opportunities
.png)





Find Collaborating Physicians

